|
Can volunteers working with sex offenders correctly predict risk?
Andrew J.P. Bates1, Nadia M. Wager2
1Principal Forensic Psychologist, National Probation Service, UK and Circles UK
2Reader in Forensic Psychology, University of Huddersfield
[Sexual Offender Treatment, Volume 12 (2017), Issue 2]
Abstract
Aim/Background: The purpose of the study was to examine the effectiveness of the Dynamic Risk Review (DRR), a quarterly-completed risk assessment profile based on 17 questions scored on a Likert scale (0-6) by volunteers who are working with Circles of Support and Accountability (CoSA) in the UK.
Methods: The case files of 447 sex offenders (known as 'Core Members') held by Circles UK were analysed to identify any 'adverse outcome' in the person's behaviour since they had taken part in a CoSA receiving community support from trained volunteers. Fifty-six such cases were identified with 'adverse outcomes' ranging from arrest but with no further charge to reconviction for a sexual offence. Thirteen Core Members with adverse outcomes were identified as having at least three DRR assessment records. These 13 Core Members were compared with a randomly selected control group of Core Members with no recorded adverse outcomes and at least three recorded DRR scores.
Results: It was observed that DRR scores for the adverse outcome group remained high while those for the control group reduced and this finding was statistically significant. Further analysis was undertaken to see which questions on the DRR were most associated with adverse outcome.
Conclusions: There is discussion about how responses to DRR questions might inform case management of Core Members by CoSA organisations in the future, and how these findings fit in with sex offender management in the community in the UK more generally.
Keywords: Circles of support, sex offender, community, risk assessment
Introduction
Circles of Support and Accountability (CoSA) is an international criminal justice/ child protection initiative which was introduced to the UK in 2002 (Bates, Williams, Wilson & Wilson, 2014), having its origins in Canada (see Wilson & Picheca, 2005). CoSA is now active in the UK, the US, the Netherlands, Spain, Ireland and Bulgaria. The essential principle of CoSA is that selected and trained volunteers from the community, guided by professional Circle co-ordinators, work with a convicted sexual offender (usually recently released from prison) known as a 'Core Member' (CM) in order to provide them with social support and guidance, while holding them accountable for their actions and to their commitment not to re-offend (Hanvey, Philpot & Wilson, 2011).
Various studies have explored the impact of CoSA to the community management of sexual offenders and reconviction (e.g. Wilson, McWhinnie & Wilson, 2008; Wilson, Picheca, & Prinzo, 2005). These studies demonstrated that the rates of sexual reoffending over an average of approximately four and a half years were five percent for 60 CoSA participants and almost seventeen percent for 60 matched comparison subjects who were not involved in a Circle. Further to this Wilson, Cortoni and McWhinnie (2009) compared recidivism outcomes between 44 CoSA participants and 44 nonparticipants who were matched on the basis of risk, length of time in the community, release date and location, and prior involvement in sex offender treatment. Similar to the results from the pilot project evaluation, they found that CoSA participation significantly reduced sexual recidivism by 83%, violent recidivism by 73%, and general recidivism by 72%.
Other evaluations have focussed on the economic benefits of COSA. Duwe (2012) reports how, in 2008, the Minnesota Department of Corrections in the US implemented Minnesota CoSA (MnCoSA). Using a randomized experimental design, Duwe's study evaluated the effectiveness of MnCoSA by conducting a cost-benefit analysis and comparing recidivism outcomes in the MnCoSA (N = 31) and control groups (N = 31). The results from Cox regression models suggest that MnCoSA significantly reduced three of the five recidivism measures examined. By the end of 2011, none of the MnCoSA offenders had been rearrested for a new sex offense, compared with one offender in the control group. Because of less recidivism observed among MnCoSA participants, the results from the cost-benefit analysis show the programme has produced an estimated US$363,211 in costs avoided to the state, resulting in a benefit of US$11,716 per participant. For every dollar spent on MnCoSA, the programme has generated an estimated benefit of US$1.82 (an 82% return on investment).
Bates et al. (2014) conducted a study of 71 Core Members supported by Circles South-East in the UK, with reference to demographic data, offense and sentencing histories, risk assessment data and considerations regarding Multi Agency Public Protection Arrangements. A group of 71 comparison subjects who were referred to the same CoSA project and deemed suitable for, but did not receive, the service was identified. The number of reconvictions for any kind of further offence, including breach of Sex Offender Registration requirements and Sex Offence Prevention Orders, for both groups over a 55-month period was identified using the UK Police National Computer. The analysis revealed that the incidence of violent and contact sexual reconvictions in the comparison group was significantly higher than for the Circles cohort. Seven violent and three contact sexual offences were committed during the follow-up period by the comparison group, whereas there were no reconvictions for sexual or violent offences for the for the Core Member group. However, reconviction for non-contact sexual offences were slightly higher for the Core Members than the comparison group (three versus two).
In 2007 Circles UK was established, a national organisation covering England and Wales which provided oversight and standardisation of CoSA practice. In seeking to evidence the efficacy of CoSA, one significant challenge was to identify a way to meaningfully monitor a CM's pathway through the circle, noting areas of positive progress but also issues of concern which might link to risk of further offending. In this regard CoSA had the same objective as other agencies working in the sex offender field e.g. to identify and systematically record a range of changeable or dynamic risk factors presented by CMs during the life of their Circle using a structured process (see Hanson & Morton-Bourgon, 2009; Andrews and Bonta, 2006).
Mann, Hanson and Thornton's (2010) findings proved helpful in this regard, since they identified a range of 'psychologically meaningful risk factors' which were identified from meta-analysis of previous studies related to sexual recidivism. Key underlying risk factors were identified as a) history of sexual violence b) negative social influences c) poor cognitive problem solving and d) loneliness. Hanson and Harris (2000) and Hanson, Harris, Scott and Helmus (2007) classified dynamic risk factors as either stable (behaviours and attitudes developed over long periods of time which are entrenched within the offender) or acute (factors that may last only hours or days) and are shown to be predictive of imminent sexual offending. These underlying principles informed the development of OASys (Offender Assessment System) from 2001 onwards within the UK's National Offender Management Service (NOMS) for undertaking a general assessment of dynamic risk of serious harm (see Moore, 2015). This wider analysis and recording of dynamic risk factors offered a more detailed risk assessment than purely actuarial processes such as Risk Matrix 2000 and was sensitive to psychological change in the offender or changes in their social and situational context.
In 2011 a further study by McGrath, Lasher and Cumming reported on a model which combined static and dynamic risk measures. Study participants were 759 adult male sex offenders under correctional supervision in Vermont, Canada who undertook community sex offender treatment between 2001 and 2007. These offenders were assessed once using static measures (Static-99R, Static-2002R and VASOR) at the date of placement in the community. A 22-item dynamic risk measure (SOTNPS) was then used to assess participants shortly after their entry into community treatment and then every six months afterwards. Analyses of SOTNPS scores resulted in the development of a new 16-item dynamic risk measure, the Sex Offender Treatment Intervention and Progress Scale (SOTIPS). At fixed one- and three-year follow-up periods from participants' initial, second, and third dynamic risk assessments, the SOTIPS showed moderate ability to rank order risk for sexual, violent, and any criminal recidivism and return to prison. Participants who demonstrated treatment progress, as reflected by reductions in SOTIPS scores, showed lower rates of recidivism than those who did not.
In order to evidence efficacy of the model, it was important that CoSA practice in the UK could also develop systems to identify relevant attitudes and behaviours observed in CMs and thereby record both an ongoing risk assessment of the CM and also progress that they were observed to make in a number of key areas. Existing mechanisms used by UK police and probation services were not deemed adequate for this purpose as their primary focus was on the observation and monitoring of risk factors alone (e.g. the 'accountability' aspect addressed by the work of CoSA) rather than the acquisition and maintaining of 'social capital' by CMs which was the additional primary aspect of CoSA's work - the 'support'. Hence CoSA needed to design and pilot its own methodology for evaluating dynamic risk.
To address this need, the Dynamic Risk Review (DRR) (Bates and Wager, 2012) was developed, a 17-item checklist designed to gather relevant risk information on CMs using questions about attitudes and behaviours which were observed by volunteers. The DRR questions are based upon the four areas of dynamic risk identified in the Structured Risk Assessment (Thornton, 2002a) and the associated Structured Assessment of Risk and Need (SARN) (Webster et al., 2006). Both of these assessment tools are currently used in the assessment of sexual offenders in UK accredited treatment programmes run by Her Majesty's Prison and Probation Services (HMPPS). The four risk domains addressed by the SARN are: - Offence-related sexual interests
- Pro-offending attitudes
- Problems in social and emotional functioning
- Self-management issues (e.g. lifestyle problems, impulsive attitudes and behaviours, substance abuse and accommodation insecurity).
CoSA activity involves and allows for discussion and analysis of all four risk domains to some extent, but the latter two in particular. This is because these risk factors may be reflected in attitudes and behaviours displayed by the CM in the everyday social situations in which the circle primarily operates (e.g. the emotional state and social functioning of the CM). For this reason, risk factors in SARN domains one and two are addressed in two DRR questions each (questions 1-4), while five DRR questions apply to Domain three (questions 5-10) and six in domain four (questions 11-17). Two additional questions relate to self-esteem and protective factors (e.g. appropriate hobbies, accommodation and employment). Each question is scored on a six-point Likert scale which add up to a total risk score for the Core Member. All the questions in the DRR are provided as an Appendix. Qualitative comments on each response are provided by the volunteers completing the DRR to support the score awarded. For example:
Question 4: Has the CM expressed hostile or negative views towards women?
0 1 2 3 4 5 6
Peter recently went for a job interview at a supermarket where he was not successful. The interviewer was a women and Peter said that he believes this is the reason why he did not get the job. He said that women aren't very good judges of character. He said he that this has put him off applying for other jobs.
Following a pilot study, the DRR was introduced to all COSA projects in UK in December 2009 (Bates & Wager, 2012). The DRR is completed quarterly on each Core Member by the Circle coordinator seeking answers to each question using the Circle volunteers as a focus group. Completion is carried out four times a year (e.g. every three months) as this was considered by Circles UK to be a reasonable expectation of such activity from Circles volunteers who are taking part in a circle in their own time. Therefore, it was considered that the requirement for a process of formal information recording was less than might be expected for a professional involved in ex-offender management. Indeed, some challenges were observed in the initial application of the DRR, such as the requirement by the coordinator to collate the opinions of a group of 3-4 volunteers regarding attitudes and behaviours observed in the CM. Not all volunteers had the same opinions about the CM and it became the Circle co-ordinator's responsibility to decide upon a score on a DRR question which most accurately reflected the summarised group opinion. It should also be noted that a less structured record of every circle meeting is kept in the form of Circle minutes which are returned to and stored by each CoSA project.
Scores for each DRR are also returned to Circles UK for central recording on a database which was accessed for the purposes of this current research. Circles UK also holds much demographic and other information on CMs drawn from COSA organisations from around the UK, which includes any incidence of 'adverse outcome' for the CM (e.g. any recorded inappropriate or illegal behaviour). Although, it should be noted that such information is not systematic, ongoing and complete for all core members, since police national computer (PNC) data relating to all reconviction is not available to CoSA projects. However, locally recorded 'adverse outcome' data might include activities which would not be recorded on the PNC as it fall below the threshold of actual reconviction (i.e. the CM being arrested for, or charged with. any new offence, subject to any child protection activities bought be a children's services or preventative action by the police ViSOR [Violent and Sex Offender Registration staff]). This information is thus the widest available record of 'adverse outcomes' for CMs. However, it should be noted that 'adverse outcome' data is primarily available for active Circles and does not usually cover longer post-circle periods when the responsible CoSA organisation may gradually lose touch with the CM.
The aim of the analysis presented in this paper was to ascertain whether the DRR scores, or at least their trends over successive assessment points, for Core Members who demonstrate adverse outcomes differ from Core Members without adverse outcomes.
Method
In December 2015 Circles UK had details of 447 CMs since CoSA inception in 2002. Of this total 56 (12%) had some kind of adverse outcome (AO) recorded against them. This data broke down as follows (N.B. outcomes are not mutually exclusive):
Arrest (for any offence) | 41 | (9%) | Recall to prison | 41 | (9%) | Other breach of licence/ community order | 39 | (8.7%) | Reconviction (for any offence) | 13 | (3%) | Recorded reconvictions (13) were broken down as follows: | Breach of Sex Offence Prevention Order (SOPO) | 9 | | Sexual assault | 2 | | Caution for sexual behaviour | 1 | | Historical sexual assault | 1 | |
The historical offence recorded pre-dated the CM's prison sentence and their subsequent time in circle.
It should be noted that the current paper is not a reconviction study per se. The information available about adverse outcomes was not exhaustive. There may have been further adverse outcomes after the Circle had ended or CoSA UK data-gathering had ceased, or even during the Circle lifetime but, which had not been reported to Circles UK. This paper seeks to identify the CMs for whom there was some kind of broadly-defined adverse outcome in order to examine if this eventuality was reflected in the DRR record to a statistically significant degree.
Of the 56 CMs with adverse outcomes, 31 had at least one DRR recorded. Totals of DRRs recorded for this group were:
1 DRR 8
2 DRRs 10
3 DRRs 10
4 DRRs 3
It was considered that a minimum of three DRR completions for a CM (e.g. over the course of a full year of Circle activity) was necessary for the purposes of meaningful analysis. This led to a sample of 13 CMs with adverse outcomes for the study. A matched sample of 13 CM with no recorded adverse outcomes was randomly selected for each AOCM. The criteria for matching was that the CM had to be from the same CoSA project and have the same number of DRRs recorded. This necessarily limited the pool of control CMs but selection of the control meeting the criteria was random. This analysis reports on the difference in trajectory between the AOCM DRRs and the control group and statistical significance of the finding.
Results
Descriptive Statistics
| Table 1: Descriptive Statistics |
|
Mean DRR1 |
Mean DRR2 |
Mean DRR3 |
| Adverse Outcomes (n = 13) |
34.08 (sd = 8.51)
CI (95%)
28.9 – 39.2
|
34.23 (sd = 11.88)
CI (95%)
27.06-41.41
|
32.54 (sd = 8.76)
CI (95%)
27.24 – 37.83 |
Matched Control (n = 13)
|
36.69 (sd = 8.16)
CI (95%)
31.76 – 41.62
|
30.15 (sd = 9.27)
CI (95%)
24.55- 35.75
|
24.85 (sd = 12.69)
CI (95%)
17.18 – 32.52 |
At the aggregate level, the matched control group (e.g. CMs without an adverse outcome) had slightly higher scores for the initial DRR, yet as a group they demonstrated an incremental decline in scores at each successive point of assessment. The same decline in scores was not observed for the group who demonstrated adverse outcomes.

| 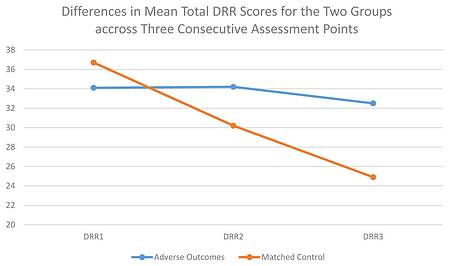
| Graph 1: DRR scores Adverse Outcome vs. Comparison Group |
Inferential statistics
Due to the relatively small sample size in this analysis non-parametric analyses were used. However, when using the total scores for the DRR assessments, with larger samples sizes it would be possible to utilise parametric analyses. This would enable the investigation of both main and interactive effects between variables simultaneously.
The first analyses were performed to determine whether each of the two groups demonstrated DRR score profiles which evidenced incremental decline in risk over time. It was hypothesised that only the comparison and not the adverse outcomes group would demonstrate an incremental decline in risk profiles. The analysis was computed after splitting the SPSS data set by group, which enabled separate analyses to be conducted for the adverse outcome and comparison groups. Freidman's test, which is the non-parametric equivalent of a repeated one-way ANOVA, revealed that there was no statistically significant decline in DRR scores over assessment periods for the adverse outcome group (Χ2 = 1.960, df = 2, p = .188). Conversely, the observed decline in DRR scores over time for the comparison group appeared to be heading towards a statistically significant difference after adjusting for Bonferroni's correction (Χ2 = 4.531, df = 2, p = .052). Post hoc analysis, using Wilcoxon's signed rank test, were then performed on paired comparisons of DRR scores for the comparison group. This revealed that comparison between both the first and second (z = -2.451, p = 0.007, r = -0.679), and the first and third (z = -2.483, p = 0.007, r = -0.688) DRR assessment scores showed statistically significant reductions over time. Both of which evidenced large effect sizes. The comparison between the second and third DRR assessment scores was heading towards statistical significance and demonstrated a medium effect size (z = -1.944, p = 0.025, r = -0.538). Thus, suggesting that an increase in sample size might lead to this finding reaching a level of statistically significant difference.
The second analyses were conducted to ascertain whether there were statistically significant differences between the adverse outcome and comparison groups in relation to their changes in DRR scores between assessment points. Initially, differences between DRR scores for each individual between assessment points one and two, two and three and one and three were computed. These differences in scores were then used as dependent variables in three Mann-Whitney U tests. The analyses revealed a trend just falling short of being a statistically significant, after adjusting the p value according to Bonferroni's correction, between the two groups based on their differences in their scores on their first and second DDR assessments. The lessening of risk was greater for the comparison group than the adverse outcomes group (U = 48.0, z = -1.879, p = 0.032, r = -0.368). This observed difference demonstrated a medium effect size, which would suggest that the finding may reach a level of statistical significance with an increase in the sample size. There was no statistically significant difference between the two groups on the basis of the differences between their scores on their second and third DRR assessments (U = 60.0, z = -1.260, p = 0.208, r = -0.247). However, the observed difference between the two groups based on their differences in their scores on their first and third DDR assessments was also indicated a trend heading towards statistical significant. The lessening of risk was greater for the comparison group than the adverse outcomes group (U = 61.0, z = -1.875, p = 0.032, r = -0.368). Again, this observed difference demonstrated a medium effect size, which would suggest that the finding may reach a level of statistical significance with an increase in the sample size.
Individual level data analysis
Cursory exploration of the individual profiles of DRR scores was undertaken to determine whether there were markedly different patterns of score profiles between the two groups. Only two of the adverse outcome group members demonstrated an incremental decline in their DRR scores and these declines, where evident, were relatively small. Additionally, a further three members of this group demonstrated decline in scores at assessment point three. In contrast seven of the matched-control group members demonstrated a marked incremental decline in scores. Within the matched control group there were four group members who demonstrated profiles that might indicate risk for an adverse outcome in the near future (c3, c4, c7, c8). In terms of ascertaining the predictive validity of the tool further it would be prudent to track this group to see whether these four individuals, and not the other nine go on to exhibit adverse outcomes.
| 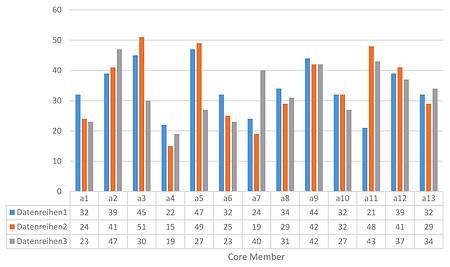
| Table 2 (Series=DRR recording occasion (quarterly)) |
| 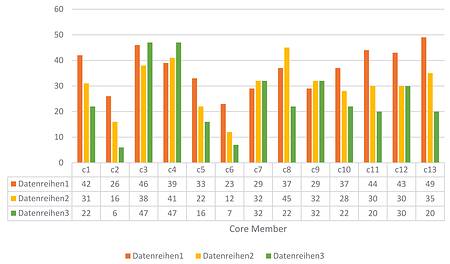
| Table 3 |
Discussion
The above findings confirm that a quarterly recorded assessment by a group of CoSA volunteers using the Dynamic Risk Review shows a meaningful association with actual problematic or adverse behaviour which was exhibited by Core Members. This is in spite of the practical challenges that have always occurred in the collection of this data. This has included the fact that the DRR information is gathered only every three months at the end of a Circle meeting (usually at around 9pm, when the volunteers are often more-than ready to go home after an evening of providing their unpaid support for the CM). Also the DRR is a compilation of opinions offered by volunteers (who may actually espouse quite different views) which is collated upon by the Circle Coordinator. This is a positive finding with regard to the public protection aspect of CoSA as it provides evidence that trained volunteers are able to meaningfully observe and record risky attitudes and behaviours in sex offenders they are working with in the community as well as provide the more obvious 'support' aspect of the Circle's function.
Limitations of the study
Although the study yielded statistically significant results and overall follows up a large number (n=447) of CoSA Core Members since 2002, the actual number who met the criteria for the study was relatively low (n=26). This was because the study focussed on CMs with an adverse outcome who had at least 3 DRRs recorded (n=13), matched with a matched number with no adverse outcome recorded against them (n=13). It would be useful to undertake further analysis of DRR scores exhibited by CMs with an without advserse outcomes to see if this finding is maintained.
Relationship with related research and practice
Alongside the developments in CoSA practice described in this paper, there are similar activities in the field of dynamic risk assessment of sex offenders in the community in the UK and beyond. This includes the development and roll-out of the Active Risk Management System (ARMS) in police ViSOR (Violent and Sexual Offender Register) units (which are responsible for the administration of the UK Sex Offender Register) and the National Probation Service. In 2008, the UK National Offender Management Service (NOMS) began a pilot of the Stable and Acute dynamic risk assessment tool (Hanson et al., 2007) in Police and Probation Services across England and Wales. This was evaluated in 2010 by McNaughton-Nicholls and colleagues. The positive aspects of the assessment tool highlighted by the evaluation included the increased awareness of critical risk issues, a more targeted response to high risk offenders and improved partnership working based on shared information. However, the evaluation also highlighted challenges in the implementation of the tool. These included regional variations in the administration of the assessment and a reported difficulty in interpreting the meaning of some items, and thereby problems in rating them effectively. Consequently, NOMS decided not to progress with the Static and Acute assessment tool, instead they developed their own dynamic risk assessment tool - Active Risk Management System (ARMS). This methodology has much in common with the DRR and at a Circles UK launch event in 2009 a representative of NOMS also gave a paper about the development and roll-out of ARMS. Thirteen factors (eight risk factors and five protective factors) were included in the ARMS assessment. Risk factors included: Opportunity to offend, offence related sexual interests, sexual pre-occupation, emotional congruence with children, hostile orientation to others, poor self-management, negative orientation to rules and anti-social influences. Protective factors included: Pro-social network, a commitment to desist, an intimate relationship, employment / being busy and a sense of citizenship / giving something back. Similar to the implementation of the DRR, the presence of each risk factor is assessed and given a priority rating. However, with ARMS the ratings indicate a risk management action (high, medium, low), depending on whether there is clear / strong evidence, some evidence or no evidence of the presence of the particular factor. The ARMS assessment has five stages and staff undertaking the assessment are expected to use a range of information sources, including interviews, observations and analysis of case files. An early evaluation of the implementation of ARMs (Webster, 2014) found that staff had found the joint-organisation aspect of training beneficial, noting that it enhanced their understanding of how ARMS was applied across different settings and roles. It was observed that the ARMS assessment process was clear, but could be lengthy to complete so they suggested a more streamlined version with fewer factors to rate overall. They also suggested that ARMS might be integrated with existing assessments such as OASys and Risk Management Plans.
Additionally, Hanson and colleagues (2017) have developed a 'Five level risk and need system' which seeks to standardise different risk assessment models into a unified whole thereby informing case management by correctional agencies as well as assessing risk. The system utilises five different categories of risk and need from Level 1 for individuals with "few, if any, identifiable criminogenic or non-criminogenic needs. Any needs they exhibit are minimal and/or transitory in nature". Through to Level 3 people with "one or two discrete criminogenic needs that are considered primary drivers of their criminal behaviour. People in Level III are also likely to "have some non-criminogenic needs typical of the general correctional population (e.g., past trauma or mental health needs). Members of this level tend to have some identifiable resources and strengths, but their needs (criminogenic and non-criminogenic) are likely to be barriers to effective use of these resources and strengths". The highest level of risk and need is Level 5 who have" most, if not all, of the major criminogenic needs from the psychological, interpersonal, and lifestyle domains. Many of these needs are chronic, severe, and longstanding. In addition, these people likely have multiple, severe, and chronic non-criminogenic needs". The Five Level Risk and Needs System recommends differing levels of case management according to identified risk and needs scores and is a coherent and thorough methodology combining a range of information relating to these two key aspects of offender risk assessment. It will be interesting to see if is more widely adopted across jurisdictions internationally.
Practical implications of the research
If it can be demonstrated that DRR scores are linked to adverse outcome in a CM it then becomes necessary to consider at what point and how should evasive action be taken with regard to risk management of the CM following a negative DRR finding?
One possibility is that DRRs might be completed more regularly by volunteers, possibly as often as every month or even after every circle meeting. This would not be feasible with the current arrangement whereby the Circle coordinator administers the DRR because contact between coordinator and circle is less regular than monthly. However, it may be possible that the DRR could be completed more regularly by the volunteers on an individual basis thereby providing a much more detailed amount of DRR data on every CM. Such a process would require significant development of information-gathering capacity for Circles organisations. One possibility here might be using more advanced information technology such as using a mobile phone app to record more regular DRR scores by volunteers, which then feeds into a centralised matrix of risk assessment information available to Circles Coordinators who would be required to note outcomes of concern and then intervene accordingly.
What directions might future research take?
Statistical limitations of the current research meant that proposed analysis of the correlation between scores on individual DRR questions at each point of recording and adverse outcomes for CMs was not viable. However, this presents an important future research question. Cases where there were two DRR completions might also be examined to contribute to such an analysis. Ideally the DRR could then be reduced to a smaller number of questions which can be shown to have particular validity in predicting adverse outcome. A shorted DRR might then, as suggested above, be completed more often on each CM to provide a much richer source of data to inform case management by CoSA agencies.
Conclusion
The current research provides evidence that the DRR is a valid tool of community risk assessment for use with CMs thereby allowing Circles projects to better enforce the 'Accountability' aspect of their work alongside the 'Support'. Wider use of this process might thus be pursued to further enhance the way in which CoSA can contribute to public protection and sex offender management in the UK.
References- Andrews, D. A., & Bonta, J. (2006). The psychology of criminal conduct (4th ed.). Newark, NJ: LexisNexis.
- Bates, A, Williams, D, Wilson, C & Wilson, R (2014) COSA South-East: The first ten years. International Journal of Offender Therapy and Comparative Criminology, 58(7): 861-885
- Bates, A. & Wager, N. (2012) Assessing Dynamic Risk in the community: The DRR and COSA of Support and Accountability, Forensic Update 108: 5-13
- Duwe, G. (2012) Preliminary results from a randomised experiment in Minnesota: Can Circles of Support and Accountability (CoSA) work in the United States? Sexual Abuse: A Journal of Research and Treatment, 25(2):143-65
- Hanson, R. K., & Harris, A. J. R. (2000). Where should we intervene? Dynamic predictors of sex offense recidivism. Criminal Justice and Behavior, 27, 6-35.
- Hanson, R.K., Harris, A.J.R., Scott, T.L. & Helmus, L. (2007). Assessing the risk of sexual offenders on community supervision: The Dynamic Supervision Project. (User Report No. 2007-05). Ottawa, Ontario: Public Safety Canada. Retrieved from www.publicsafety.gc.ca/cnt/rsrcs/pblctns/ssssng-rsk-sxl-ffndrs/index-eng.aspx
- Hanson, R. K., & Morton-Bourgon, K. E. (2009). The accuracy of recidivism risk assessments for sexual offenders: A meta-analysis of 118 prediction studies. Psychological Assessment, 21:1-21
- Hanson, R. Karl, Guy Bourgon, Robert J. McGrath, Daryl Kroner, David A. D'Amora, Shenique S. Thomas, Lahiz P. Tavarez, (2017) A Five-Level Risk and Needs System: Maximizing Assessment Results in Corrections through the Development of a Common Language (New York: The Council of State Governments Justice Center).
- Hanvey, S., Philpot, T., & Wilson, C. (2011). A community-based approach to the reduction of sexual reoffending: CoSA of Support and Accountability. London, England: Kingsley.
- Mann, R., Hanson, K. & Thornton, D. (2010). Assessing risk for sexual recidivism: Some proposals on the nature of psychologically meaningful risk factors. Sexual Abuse: A Journal of Research and Treatment, 22(2):191-217
- McGrath, R., Lasher, M. & Cumming, G. (2011). A model of static and dynamic sex offender risk assessment. Report for the U.S. Department of Justice
- McNaughton Nicholls, C., Webster, S. & NatCen Social Research Crime and Justice Team (2014). Sex Offender Management and Dynamic Risk: Pilot evaluation of the Active Risk Management System (ARMS). Ministry of Justice Analytical Series
- Moore, R. (ed) A compendium of research and analysis on the Offender Assessment System (OASys) 2009-2013 , Ministry of Justice Analytical Series July 2015
- Thornton, D. (2002) Constructing and testing a framework for dynamic risk assessment. Sexual Abuse: A Journal of Research and Treatment, 14(2):137-151.
- Webster, S. D., Mann, R. E., Carter, A. J., Long, J., Milner, R. J., O'Brien, M. & Ray, N. (2006). Inter-rater reliability of dynamic risk assessment with sexual offenders. Psychology, Crime & Law, 12(4): 439-452.
- Wilson, R. J., & Picheca, J. E. (2005). Circles of Support and Accountability: Engaging the com¬munity in sexual offender risk management. In B.K. Schwartz (Ed.), The sex offender (Vol. 5). Kingston, NJ: Civic Research Institute.
- Wilson, R.J., Picheca, J.E. & Prinzo, M. (2005). Circles of Support and Accountability: An evaluation of the pilot project in South-Central Ontario (Research Report R-168), Ottawa, ON.: Correctional Service of Canada.
- Wilson, R. J., McWhinnie, A. J., & Wilson, C. (2008). Circles of Support & Accountability: An international partnership in reducing sexual offender recidivism.
- Prison Service Journal, 138:26-36
- Wilson, R. J., Cortoni, F., & McWhinnie, A. J. (2009). Circles of Support and Accountability: A Canadian national replication of outcome findings. Sexual Abuse: A Journal of Research & Treatment, 21(4): 412-430.
- Wilson, R.J. & McWhinnie (2016) in Circles of Support & Accountability: The Role of the Community in Effective Sexual Offender Risk Management in A. Phenix, & H.M. Hoberman (eds.), Sexual offending: Predisposing antecedents, assessment and management. New York: Springer
Appendix - The Dynamic Risk Review
Questions 1-15 invite a numerical response graded 0-6 on a Likert scale as well as additional supportive qualitative information.
A. Sexual Interests- Is there evidence that the CM is struggling with problematic sexual thoughts?
E.g. Has the CM expressed a sexual preference for children or an offence related sexual interest? - Has the CM spoken to an excessive and/or inappropriate degree about sexual matters in general?
E.g. Sexualisation of non-sexual situations,
Focusing on sexual aspects of a situation
Excessively talking about sex
B. Offence Related Attitudes- Has the CM expressed any sexualised attitudes towards children?
E.g. Has the CM expressed that children can flirt with adults, know a lot about sex are not as innocent as people think, and are not harmed by sexual contact with adults? - Has the CM expressed hostile or negative views towards women?
E.g. Does the CM believe women play psychological games, are manipulative or untrustworthy people?
C. Relationships- Is there any evidence that the CM is displaying a high level of emotional identification with children?
E.g. Does he believe that he gets on better/feels more comfortable with children than adults? Is he hanging round places where children tend to hang around? - Is there evidence that the CM is experiencing feelings of emotional loneliness?
E.g. Core Member stated that they have no friends or that they feel lonely - Is there evidence that the CM is experiencing feelings of inadequacy in relationships?
E.g. That they find it difficult to get close to others
That they are not good enough or deserving of love
That they struggle with relationships - Does the CM have stable emotional relationships with any other people outside the Circle?
E.g. The CM has close friendships that are appropriate
They are romantically involved with someone appropriate
D. Self-management - Is there evidence that the CM is experiencing feelings of powerlessness or hopelessness?
E.g. They feel that they do know how to solve life's problems
They feel that nothing they do is right
They feel that they aren't in control of their life
Has the CM disclosed, or been observed, acting in an under assertive manner? - Has the CM demonstrated reckless behaviour?
E.g. There is evidence that the CM is abusing drugs or alcohol.
Have they put themselves in situations that are potentially risky?
Is the CM being financially irresponsible?
Is the CM frequently changing jobs? - Has the CM expressed any hostile feelings or angry outbursts?
E.g. Does CM display emotional extremes?
Has the CM been withdrawn, isolated, over controlled, aggressive or impulsive? - Does the CM demonstrate appropriate problem solving abilities?
E.g. The CM uses proactive approach to problem solving - Does the CM maintain realistic relapse prevention strategies?
E.g. The CM recalls and refers to the work they have done in Relapse Prevention work they did during treatment?
E. Additional questions- Is there evidence that the CM is experiencing any feelings of low self-esteem?
E.g. Feeling that they are not good enough
Has the CM lacked motivation to do things?
Poor view of themselves? - Does the CM engage in appropriate activities and hobbies?
E.g. Pub darts, reading club, etc.
NOTE - What is appropriate for one Core Member might not be appropriate for another. The Coordinator will need to make a judgement on whether the activity or hobby is appropriate or not.
The following 2 questions invite a YES/NO response. - Is the CM in stable and suitable accommodation?
E.g. Are they homeless?
(Living in a hostel would be considered as stable)
Does their accommodation frequently change? - Is the CM involved in any paid or voluntary work?
E.g. Does the CM get satisfaction from work?
Author address
Andrew Bates
National Probation Service
South-West/South Central Division
Head Office
Kingsclere Road
Bicester
Oxfordshire
OX26 2QD
andrew.bates18@btopenworld.com
|