|
Co-Morbid Mental Disorders in Incarcerated Paedophiles
Tony Adiele1, Christopher M. Davidson2, Michael C. Harlow2, Elena del Busto3
1 Advanced Forensic Psychiatry & Medical Law Service, Cambridge, UK
2 Sanford School of Medicine, University of South Dakota, USA
3 Department of Psychiatry, University of Pennsylvania School of Medicine, USA
[Sexual Offender Treatment, Volume 6 (2011), Issue 2]
Abstract
While considerable research has been conducted regarding paedophilia, there is a paucity of research about the mental health issues of incarcerated paedophiles. This study involved 70 inmates at the South Dakota State Prison who met DSM-IV paedophilia classification requirements for age and duration of sexual interest towards prepuberal children. Study participation was voluntary and subjects were not financially compensated. Study subjects completed the Millon Clinical Multi-axial Inventory- 3rd Edition (MCMI-III). A high percentage of subjects displayed co-morbidity for Axis I and Axis II disorders. The most common Axis I disorders were Generalized Anxiety Disorder and Alcohol Abuse. The most prevalent DSM- IV Axis II disorder was Avoidant Personality Disorder. The observed high co-morbidity levels were lower than, but comparable to previous data of incarcerated child molesters and prior data of co-morbid disorders in non-incarcerated paedophiles. However, as participation was voluntary, participation bias may have affected score outcomes.
Key words: Sex Offenders, Paedophilia, Personality disorders, Prison, Co-morbid mental disorders, Millon Clinical Multi-axial Inventory, DSM-IV
Introduction
Child sexual abuse is a problem of daunting proportions in most parts of the world. In one general population study of American adults, 12% of men and 17% of women reported having been sexually abused by an older person when they were children (Fagen, Wise, Schmidt & Berlin, 2002). Given the constellation of child sex offender typologies (Eher, Neuwirth, Fruehwald & Frottier, 2003), paedophilia is of prime note as these individuals exhibit a preference for children as their primary sexual interest. Paedophiles display high levels of psychological fixation towards children as sexual partners, a primary factor in paedophile sexual recidivism (Fagen et al., 2002).
The proportion of child sex offenders who meet Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision, 2000 (DSM- IV-TR) criteria for paedophilia is estimated at 25%-45% (Fagen et al., 2002). DSM-IV criteria for paedophilia require (1) that the individual has exhibited, for at least six months, recurrent and intrusive sexually arousing fantasies, urges, or behaviors involving a child 13 years or younger; (2) these sexual fantasies, urges, or behaviors cause clinically significant distress or impairment in social, occupational, or other important areas of functioning; and (3) the person is at least 16 years of age and at least five years older than the child in question. Further DSM-IV qualifiers include if a paedophile is sexually attracted to one or both genders, if the paedophile victim is one of incest, or if the paedophile is exclusively attracted to children (Bickley & Beech, 2001).
The current DSM-IV classification system for paedophilia has been criticized for potentially excluding "child molesters" who are sexually fixated on children. The DSM-IV criteria requiring "current and intense" sexual features, lacks clarity and is open to clinical interpretation (Bickley & Beech, 2001). Also, the requirement of sexual fixation towards children for six months generates a clinically skewed view as many paedophiles dissimulate the true scope of their sexual urges (Bickley & Beech, 2001). This reticence may be considerable when paedophiles are motivated to avoid the legal and interpersonal consequences of their sexual fixations (Sewell & Salekin, 1997).
Individuals with paedophilic traits have been associated with co-morbid psychiatric disorders. Such co-morbidities may contribute to paedophile sexual recidivism (Fagen et al., 2002). In one study of non-incarcerated paedophile sex offenders, 93% of paedophiles displayed a minimum of one lifetime DSM-IV Axis I disorder, while 60% qualified for a DSM-IV Axis II disorder (Raymond, Coleman, Ohlerking, Christenson & Miner, 1999). In this study, the most common Axis I disorders were mood and anxiety disorders, while the most common Axis II category was Cluster C personality disorder (Raymond et al., 1999).
There is a marked shortage of clinical data regarding the prevalence of co-morbid Axis I and Axis II disorders in incarcerated paedophiles. In a case-controlled study based on the Swedish National Registers (Fazel, Sjöstedt, Langström & Grann, 2007), sex offenders were found to have a significantly increased probability of suffering from a severe mental illness compared to the general population with an odds ratio of 4.8 for schizophrenia (95% CI 3.4 - 6.7). Also, after adjustment for demographic and socio-economic confounders, sex offenders were found to be about six times more likely to have a history of psychiatric hospitalization when compared with the general population (OR 6.3, 95% CI 5.7 - 6.9).
However in an effort to understand more clearly the mental health needs of paedophiles in prison, our research study goal was to evaluate incarcerated paedophile demographics and DSM-IV Axis I/Axis II co-morbidities. We hypothesized that incarcerated paedophiles would display elevated levels of DSM-IV Axis I mood and anxiety disorders, along with Axis II Cluster C diagnoses. We completed a systematic review of potential study subjects' public and prison records to determine study eligibility. By conducting standardized psychological testing of study subjects, we examined the prevalence of incarcerated paedophile co-morbid psychiatric pathology.
Materials and Methods
This research project was approved by the Human Subject Research Review Board of the South Dakota Department of Corrections, and the Sanford School of Medicine University of South Dakota Department of Psychiatry Institutional Review Board.
Subjects
Our research study selected subjects currently incarcerated in the South Dakota Prison system that met DSM-IV criteria for paedophilia at time of offense. Age and duration of sexual fixation towards children criteria for paedophilia were determined utilizing the South Dakota state sex offender data base and state review of pre-sentencing reports. Study subjects had been convicted of sex crimes against children including rape, incest, sexual abuse, criminal sexual conduct, aggravated sexual assault, and sexual contact with a child. All study subjects were either currently or previously enrolled in the South Dakota sex offender treatment program for paedophiles.
Three South Dakota prisons held 282 inmates who met screening criteria for paedophilia. Inmates classified as special needs due to mental retardation or severe psychosis, or resided at prison sites not accessible to researchers due to extreme travel distance or lack of available testing facilities were excluded from eligibility. Of the 152 eligible inmates available for study participation, 70 subjects completed study testing. Study participation was voluntary, subjects were not financially compensated for study participation, and participation had no affect on study subjects' sentences.
Measures
The Millon Clinical Multi-axial Inventory-III (MCMI-III) was administered to all study subjects. The MCMI-III is a widely utilized test for psychiatric disorders. It includes several personality disorder scales, Axis I scales, and validity scales. The MCMI-III has been validated in both corrections and non-corrections settings (Ahlmeyer, Kleinsasser, Stoner & Retzlaff, 2003). MCMI-III diagnoses are consistent with but not isomorphic to, corresponding DSM-IV disorders (Ryder & Wetzeler, 2005). The MCMI- III has displayed high levels of sensitivity and specificity under field conditions (Ryder & Wetzeler, 2005).
This test utilizes 175 true/ false statements with the test written at the eighth grade level. Test scores are expressed in terms of base rates. Scores from 75-84 indicate clinically significant psychopathology, while scores at or above 85 suggest high probability for a clinical disorder (Retzlaff, Stoner & Kleinsasser, 2002).
Procedure
After study subjects were informed verbally and in writing regarding the study's purpose and conditions, subjects provided written informed consent. Subjects were then randomly assigned a research number known only to the subject and the on-site researcher. Completed MCMI-III answer keys coded with the subject's research number as an identifier, were computer scored by the Pearson Assessment Company.
Processed score reports were compiled by a second researcher devoid of study subject contact. Data was correlated for demographics, score ranges of 75-84, and scores of 85 or greater. Statistical analysis was completed using SPSS V.11 software. Bi-variate associations were assessed using Spearman's Rank Correlation and the Chi Squared tests, with P<.05 for determination of significance.
Results
For the 70 of 152 potential subjects that completed testing, three subjects delivered invalid scores. Subjects who participated were similar to eligible inmates who declined study participation in relation to age, marital status, race, and age of victim at time of offense. The majority of study subjects ranged in age from 20-77 years at time of offense. Study subjects had a median education level of 12 years. Victim's age at time of offense ranged from 2-13 years with the most common age group among 6-10 year old victims.
Table 1: Characteristics of Millon
Participants |
| Characteristic |
Number
(percent) or
Median (range) |
Age at time of study (N = 70)
Median yrs (range)
20-29 yrs
30-39 yrs
40-49 yrs
50-59 yrs
60-77 yrs |
44 (20-77)
9 (13%)
10 (14%)
30 (43%)
16 (23%)
5 ( 7%)
|
Race/Ethnicity (N = 70)
Caucasian
Native American
Hispanic
African American |
63 (90%)
5 ( 7%)
1 ( 1%)
1 ( 1%)
|
Education (N = 67)
Median yrs (range)
Primary
Some HS
HS grad
Post-secondary |
12 (7-20)
7 (10%)
20 (30%)
22 (33%)
18 (27%)
|
Marital status (N = 69)
Single
Married
Divorced
Widowed/Separated |
24 (35%)
14 (20%)
26 (38%)
5 ( 7%)
|
Age of victims (N = 70)
Median yrs (range)
2-5 yrs
6-10 yrs
11-13 yrs
|
9 (2-13)
14 (20%)
33 (47%)
23 (33%)
|
| Percentages may not sum to 100% due to rounding. |
Data analysis failed to determine any correlations of significance between age of offender at time of offense, race of offender, offender education level, and offender marital status compared with age of victim at time of offense. There was a trend towards significance regarding years of education among study subjects (p=0.09). This variable also correlated with age of the victim.
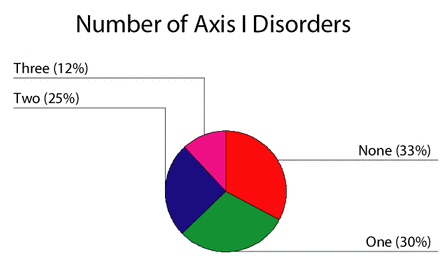
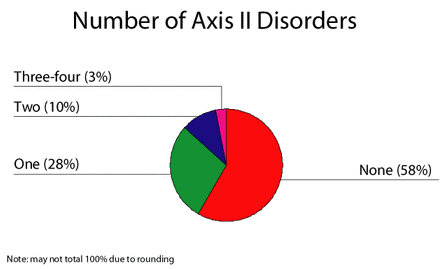
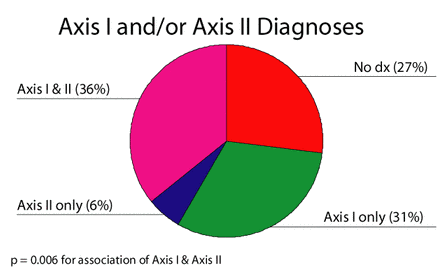
Axis I disorders occurred in 67% of test subjects with 37% meeting criteria for more than one Axis I disorder. Co-morbid Axis II disorders occurred in 42% of test subjects, with 13% of test subjects displaying more than one DSM-IV disorder. A total of 73% of test subjects met criteria for an Axis I disorder, an Axis II disorder, or a combination of Axis I and Axis II disorders.

| | Figure 1 |
| | Figure 2 |
| | Figure 3 |
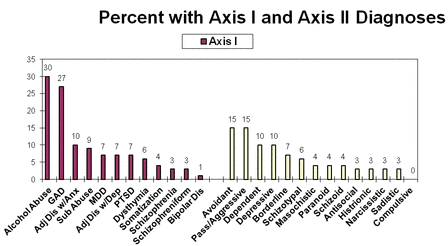
The most prevalent Axis I disorders displayed were Alcohol Abuse (30%) and Generalized Anxiety Disorder (27%). Overall, subjects displayed markedly elevated levels of pathology for various anxiety and mood disorders.
Table 2: Axis I Diagnoses |
| Diagnosis |
Number
of Participants |
With
Diagnosis Percent |
| Any Axis I Diagnosis |
45 |
67% |
| Alcohol Abuse |
20 |
30% |
| Generalized Anxiety Disorder |
18 |
27% |
| Adjustment Disorder with Anxiety |
7 |
10% |
| Psychoactive substance abuse |
6 |
9% |
| Major Depressive Disorder |
5 |
7% |
| Adjustment Disorder with Depression |
5 |
7% |
| Post Traumatic Stress Disorder |
5 |
7% |
| Dysthymia |
4 |
6% |
| Somatization |
3 |
4% |
| Schizophrenia |
2 |
3% |
| Schizophreniform |
2 |
3% |
| Bipolar Disorder |
1 |
1% |
For Axis II disorders, the most commonly observed DSM-IV personality disorder cluster was Cluster C, with Avoidant Personality Disorder (15%) and Dependent Personality Disorder (10%) the most prevalent. Millon testing categories for non-DSM-IV personality disorders included Passive-Aggressive Personality Disorder (15%) and Depressive Personality Disorder (10%).
Table 3: Axis II Disorders |
| Diagnostic Category |
Number
of Subjects
with Disorder |
Percent |
Cluster A
Paranoid
Schiziod
Schizotypal |
3
3
4
|
4%
4%
6%
|
Cluster B
Antisocial
Borderline
Histrionic
Narcissistic |
2
5
2
2
|
3%
7%
3%
3%
|
| Cluster C
Avoidant
Dependent
Compulsive |
10
7
0
|
15%
10%
0%
|
| Non-DSM-IV
Depressive
Sadistic
Masochistic
Negativistic*
(*Passive-Aggressive)
|
7
2
3
10
|
10%
3%
4%
15%
|
| | Figure 4 |
MCMI-III testing of study subjects revealed markedly elevated base rate scores between 75 and 84, consistent with MCMI-III Axis II features. Axis II Cluster B and Cluster C features occurred equally in 28% of subjects. Cluster C dependent and avoidant features were elevated at 10% and 9%, respectively. Cluster B narcissistic personality features was the largest personality typology in study subjects, occurring in 13% of subjects. Among non-DSM-IV personality types tested by the Millon-III, depressive personality type was most represented with 13% of subjects displaying these features. When rates of Axis II features were combined with Axis I and Axis II disorders, 66 of the 67 study subjects who delivered valid MCMI-III scores displayed evidence of co-morbid psychopathology.
Table 4: Axis II Features |
| Diagnostic Category |
Number
of Subjects
with Disorder |
Percent |
Cluster A
Paranoid
Schiziod
Schizotypal |
4
8
6
|
6%
12%
9%
|
Cluster B
Antisocial
Borderline
Histrionic
Narcissistic |
8
2
0
9
|
12%
3%
0%
13%
|
| Cluster C
Avoidant
Dependent
Compulsive |
6
7
6
|
9%
10%
9%
|
| Non-DSM-IV
Depressive
Sadistic
Masochistic
Negativistic*
(*Passive-Aggressive)
|
9
5
4
0
|
13%
7%
6%
0%
|
Analysis for correlations of significance for Axis I disorders displayed statistically significant correlations among mood disorders, with anxiety disorders, and between typologies of mood and anxiety disorders. Within Axis II disorders, a correlation between Negativistic Personality Disorder and Paranoid Personality Disorder was observed. Axis I /Axis II correlations occurred for mood and anxiety disorders with Cluster C personality disorders, most prominently with Avoidant and Dependent Personality Disorders. Posttraumatic Stress Disorder also displayed a high degree of correlation among subjects with co-morbid Borderline Personality Disorder.
Table 5: Significant Associations
of Axis I/Axis I and Axis II/Axis II Disorders |
| Diagnostic Category |
Correlation
Coefficients |
P-value (<.05) |
| Axis I/I |
| Adjustment Disorder with Anxiety and Major Depressive
Disorder |
.28 |
.020 |
| Post Traumatic Stress Disorder and Generalized Anxiety
Disorder |
.34 |
.003 |
| Schizophreniform Disorder and Post Traumatic Stress
Disorder |
.62 |
.000 |
| Axis II/II |
| Negativistic Personality Disorder andParanoid Personality
Disorder |
.28
|
.018
|
Table 6: Significant Associations
of Axis I and Axis II Disorders
|
| Diagnostic Category |
Correlation
Coefficients |
P-value (<.05) |
| Axis I/II |
| Alcohol Abuse and Negativistic Personality Disorder |
.28 |
.017 |
| Adjustment Disorder with Anxiety and Negativistic Personality
Disorder |
.27 |
.023 |
| Adjustment Disorder with Depression and Avoidant Personality
Disorder |
.36 |
.002 |
| Adjustment Disorder with Depression and Masochistic
Personality Disorder |
.47 |
.000 |
| Bipolar Disorder and Dependent Personality Disorder |
.27 |
.024 |
| Bipolar Disorder and Schizotypal Personality Disorder |
.32 |
.006 |
| Dysthymia and Negativistic Personality Disorder |
.25 |
.036 |
| Generalized Anxiety Disorder and Dependent Personality
Disorder |
.36 |
.002 |
| Generalized Anxiety Disorder and Schizotypal Personality
Disorder |
.24 |
.046 |
| Schizophrenia and Schizotypal Personality Disorder |
.46 |
.000 |
| Schizophrenia and Borderline Personality Disorder |
.24 |
.049 |
| Schizophreniform Disorder and Avoidant Personality |
.35 |
.003 |
| Schizophreniform Disorder and Borderline Personality
Disorder |
.50 |
.000 |
| Schizophreniform Disorder and Dependent Personality
Disorder |
.34 |
.004 |
| Psychoactive Substance Abuse and Sadistic Personality
Disorder |
.25 |
.041 |
| Major Depressive Disorder and Sadistic Personality Disorder |
.29 |
.017 |
| Post Traumatic Stress Disorder and Avoidant Personality
Disorder |
.23 |
.020 |
| Post Traumatic Stress Disorder and Borderline Personality
Disorder |
.63 |
.000 |
Post Traumatic Stress Disorder and Dependent Personality
Disorder
|
.29
|
.015
|
Discussion
Previous studies have reported high rates of co-morbid Axis I and Axis II disorders in non-incarcerated paedophile sex offenders. In the Raymond et al. (1999) study of 45 outpatient paedophile sex offenders, 93% of offenders had a diagnosis of at least one lifetime Axis I disorder other than paedophilia, with 67% of subjects having at least one Axis II personality disorder.
In the Raymond et al. (1999) study, the most prevalent co-morbid Axis I disorders were mood disorders (67%), anxiety disorders (64%), and substance abuse disorders (60%). The most common personality disorders were Avoidant Personality Disorder (25%) and Antisocial Personality Disorder (22.5%), with Cluster C personality disorders (42%), the largest personality disorder cluster.
In comparison to this non-incarcerated paedophile sex offenders, our study 's co-morbidity rates, while lower than the rates reported by Raymond et al. (1999), were still comparable in distribution of Axis I and Axis II disorders. Our study's total Axis I and Axis II disorders had lower rates at 67% and 42%, respectively. Our study's rates of mood disorders (38%), anxiety disorders (34%), and substance abuse disorders (39%), were also lower than those observed by Raymond et al. (1999).
However, these Axis I disorder categories were elevated compared to other Axis I categories for both our study and the outpatient paedophile sex offender study. Although our study's overall percentage of personality disorders at 42% is lower than the Raymond et al. (1999) reported rates, our study is consistent for rates of Cluster C personality disorders as the most elevated personality disorder cluster in both study groups. In addition, rates for Passive-Aggressive, Dependent, and Avoidant Personality Disorders were similar in both studies. The most prominent divergence in personality disorder distributions were the outpatient paedophile sex offender rates for Obsessive-Compulsive Personality Disorder (25%) and Antisocial Personality Disorder (22.5%) in Raymond et al. (1999), compared with our study's respective rates of 0% and 3%.
There are a number of potential explanations for the higher Axis I/Axis II co-morbidity rates reported by Raymond et al. (1999) compared with our study. The Raymond et al. (1999) study utilized the Structured Clinical Interview for DSM-IV disorders, Patient Edition (SCID-P) to assess paedophile co-morbidities. The SCID-P is a structured interview that tests for lifetime history of Axis I disorders as well as Axis II disorders.
In contrast, the MCMI-III true/false statements focus on contemporaneous Axis I disorders, along with Axis II disorders. These fundamental differences, along with the SCID-P lacking validity scales to rule out over-endorsement of symptoms, could result in higher Axis I disorder scores with the SCID-P instead of the MCMI-III. Also, the higher substance abuse rates reported by Raymond et al. (1999) could be explained by outpatient paedophiles having better access to drugs and alcohol than in a correctional setting. The disparity in corresponding Axis II rates could also be a reflection of inherently different types of sample pools with different motivations for study participation, particularly since the outpatient paedophile study subjects were financially compensated, while the incarcerated paedophile study subjects were not financially compensated for their participation.
Although our study utilized the MCMI-III with incarcerated paedophiles, potential parallels can be drawn with a Colorado Department of Corrections study that used the MCMI-III to test 474 sex offenders convicted of general sex crimes against minors, as part of these offender's mandatory prison intake process (Ahlmeyer et al., 2003). The authors reported that this study utilized MCMC-III base rate scores of 75 and greater to define Axis I and Axis II disorders. They observed that these study subjects displayed markedly elevated mood disorder (41%) and anxiety disorder (60%) rates at higher but comparable rates to our study's co-morbid mood and anxiety disorders.
Ahlmeyer et al. (2003) also observed that study subjects had elevated rates of Axis II Cluster A, B, and C disorders, with Cluster C typology being the most frequent. Schizoid, Antisocial, and Avoidant Personality Disorders were most frequent for each of their respective personality cluster groupings. Furthermore, Avoidant Personality Disorder was most prominent, occurring in 41% of study subjects. These most prevalent personality disorders directly correspond to observed personality disorder scores in our study, upon adjusting our study's Axis II disorder rates to include base rate scores at or above 75.
The different co-morbidity levels between these two studies could have occurred due to a variety of factors. A prime distinction is that our study focused on incarcerated paedophiles, not generalized incarcerated sex offenders against minors. The study by Ahlmeyer et al. (2003) was compulsory and administered to all offenders at time of incarceration, while our study subject's participation was voluntary and was administered at various lengths of time into each study subject's sentence. These factors potentially resulted in markedly different sample pools with different levels of co-morbid Axis I and Axis II disorders.
The lack of correlations between paedophile demographics and age of victim is consistent with previously published research, concluding that paedophile demographics, in relation to age of victims, offer a constellation of typologies. The relatively high median years of education (12years) for study participants, with low education level offenders declining study participation, are plausible explanations for the trend towards significance in offender education levels. While only 7% of study subjects were Native American, this participation is remarkable as no studies on incarcerated Native American paedophile Axis I/Axis II co-morbidities have yet been published. Further study of this underreported group of paedophiles is warranted.
Axis I/Axis I correlations display significance with anxiety and depressive disorders, in accordance with the previously documented relationship between these two co-morbidities. Although Schizophreniform Disorder correlated with Posttraumatic Stress Disorder (P<.05), the small sample size of Schizophreniform Disorder (n=2) is likely to result in an unstable sample group. The displayed Axis II correlations of Negativistic Personality Disorder (Passive Aggressive) and Paranoid Personality Disorder may reflect the previously documented elevated incidence rate of Negativistic Personality Disorder in paedophiles (Raymond et al., 1999), combined with paranoid symptoms secondary to incarceration stressors.
Axis I/Axis II correlations of anxiety disorders with Cluster C personality disorders is concurrent with similar co-morbidities reported in paedophiles. Study subjects' correlation of significance between Posttraumatic Stress Disorder and Borderline Personality Disorder is of interest given the high occurrence rates of sexual abuse among individuals with either paedophilia or Borderline Personality Disorder.
Our study group's correlations for substance abuse disorders with Cluster B and Cluster C disorders have been previously reported for both non-incarcerated paedophiles (Raymond et al., 1999) and for incarcerated general sex offenders against minors (Ahlmeyer et al., 2003). The correlation between mood disorders and Sadistic Personality Disorder also has been previously documented with incarcerated child sex offenders (Timmerman & Emmelkamp, 2001). While several correlations were observed between Schizophrenia and Schizophreniform Disorder with a variety of personality disorders, small sample sizes for Schizophrenia (n=2) and Schizophreniform Disorder suggest additional unstable Axis I disorder sample groups correlated with Axis II disorder study samples.
Our study had the limitation of a relatively small samples size. Since inmates with severe psychosis resided at locations unavailable for testing, the pool of study subjects was disproportionally low in psychotic illness thought process co-morbidities. As study participation was voluntary, participation bias may have occurred. This potentially confounding variable was possibly observed in some inmate's profound reticence to participate in our study. Such reluctance was displayed particularly among potential study subjects with self-reported low education levels or high levels of dissimulation regarding their classification as sex offenders.
Our study protocol utilized state paedophile treatment program screenings of pre-sentence reports for time criteria of paedophile urges, fantasies, or behaviors with pre-pubescent children. This use of state screenings occurred due to victim and witness confidentiality issues. While reliance on a prior review of study subjects has potential for error, this state classification for all study subjects was consistent with all study subjects meeting other criteria for paedophilia. Given previously published high rates of dissimulation among paedophiles regarding paedophilic urges and behaviors, collateral documentation of paedophilic activity was warranted to determine if individual offenders met diagnostic criteria for paedophilia.
The high levels of co-morbid Axis I and Axis II disorders displayed by study subjects are noteworthy given the relationship between paedophile co-morbid psychiatric disorders and sex crime re-offense (Fagen et al., 2002). Our study's results offer evidence that the MCMI-III is a useful resource for psychiatric co-morbidity research of incarcerated paedophiles. Our study hypothesis that incarcerated paedophiles suffer from elevated levels of mood disorders, anxiety disorders, and Cluster C personality disorders was confirmed.
Study subjects' elevated Axis I/Axis II disorders and the lack of pertinent research mandate further study of incarcerated paedophile psychiatric co-morbidities, utilizing the MCMI-III. Subsequent studies would benefit from larger sample size to improve study power. Increased study power could better delineate frequencies and distributions of co-morbid disorders. Increased sample size could also offer more statistically stable sample groups for correlation. The pronounced degree of Axis I and Axis II co-morbidity in this study supports a conclusion that incarcerated paedophiles have substantial mental health issues meriting treatment.
Acknowledgments
The authors would like to thank Dr. Clare Maxwell for her assistance with SPSS v. 11 instruction.
In addition, the authors would like to thank Dr. Adèle Harlow for typing assistance.
References- Fagen, P.J., Wise, T.N., Schmidt, C.W. jr, & Berlin, F.S. (2002). Pedophilia. JAMA 288(19):2458-2465.
- Eher, R., Neuwirth, W., Fruehwald, S., & Frottier P. (2003). Sexualization and lifestyle impulsivity:clinically valid discriminators in sexual offenders. International Journal of Offender Therapy and Comparative Criminology 47(3):452-467.
- Bickley, J.A, & Beech, A.R. (2001). Classifying child abusers:Its relevance to theory and clinical practice. International Journal of Offender Therapy and Comparative Criminology 45(1):51-66.
- Sewell, K.W, & Salekin, R.T. (1997). Understanding and detecting dissimulation in sex offenders, in Clinical Assessment of Malingering and Decpetion. Edited by Rogers R. New York:Guilford Press, PP 328-350.
- Raymond, N.C., Coleman, E., Ohlerking, F., Christenson, G.A., & Miner, M. (1999). Psychiatric comorbidity in paedophilic sex offenders. The American Journal of Psychiatry 156(5):786-788.
- Ahlmeyer, S., Kleinsasser, D., Stoner, J., & Retzlaff, P. (2003). Psychopathology of incarcerated sex offenders. Journal of Personality Disorders 17(4):306-318.
- Ryder, A.G., & Wetzeler, S. (2005). Validity of the MCMI-III in the description and diagnosis of psychopathology, in New Directions in Interpreting the Millon Clinical Multiaxial Inventory-III. Edited by Craig RJ. Hoboken, New Jersey:John Wiley & Sons, PP 248-271.
- Retzlaff, P., Stoner, J., & Kleinsasser, D., (2002). The use of the MCMI-III in the screening and triage of offenders, International Journal of Offender Therapy and Comparative Criminology 46(3):319-332.
- Timmerman, I.G., & Emmelkamp, P.M. (2001). The prevalence comorbidity of axis I and axis II pathology in a group of forensic patients, International Journal of Offender Therapy and Comparative Criminology 45(2):198-213.
- Fazel, S., Sjöstedt, G., Långström, N., & Grann, M. (2007). Sexual offending and the risk of severe mental illness. Journal of Clinical Psychiatry, 68(4):588-94.
Author address
Dr. Tony Adiele
Director
Advanced Forensic Psychiatry & Medical Law Service LLC
Suite D, South Cambridge Business Park
Cambridge CB22 3JH
Phone: +44 (0) 7737 146 437
dysgenesis@yahoo.co.uk
|